- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Nervous system
- Respiratory system
- Digestive system
- Lymphatic system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
Large intestine
The large intestine (Latin: intestinum crassum) or large bowel is the final part of the gastrointestinal tract positioned in the abdominal and pelvic cavities. It is a continuation of the small intestine, starting at the ileocecal junction and ending with the anus. The length of the large intestine measures up to 5.7 feet (1.75 meters) in adults.
The primary functions of the large intestine include the absorption of the remaining water, electrolytes from the gut contents (chyme), formation and storage of feces and subsequent expulsion in a process known as defecation. Also, the large intestine houses great amounts of gut microflora.
Note: Chyme is a thick semi-fluid mass of partially digested food mixed with digestive secretions of the stomach and intestines.
The large intestine may be divided into the following parts:
- Cecum and vermiform appendix
- Colon (ascending, transverse, descending and sigmoid)
- Rectum
- Anal canal
Characteristic features of large intestine
The large intestine differs from the small intestine with the following characteristic features:
- As the name suggests, the diameter of the large intestine is greater than that of the small intestine.
- The outer muscular layer of the large intestine forms three narrow longitudinal bands known as taeniae coli.
- The wall of the large intestine is arranged into small segmented pouches called haustra that are caused by sacculation of the large intestine.
- The outer surface of the large intestine along the free and omental taeniae has epiploic appendices that are small fat-filled projections of the peritoneum.
The taeniae coli are more pronounced on the cecum and colon and become less visible towards the rectum. Closer to the distal sigmoid colon and at the rectosigmoid junction, fibers of all taeniae become scattered, forming a continuous longitudinal muscular layer that encircles the rectum. The taeniae of the cecum converge at the base of the vermiform appendix, making it easier for a surgeon to localize it during surgery. Overall, the large intestine has three types of taeniae:
- Mesocolic taeniae - located posteromedially; correspond to the attachment of the mesentery; the transverse mesocolon and sigmoid mesocolon attach to them;
- Omental taeniae - situated posterolaterally and serve for the attachment of the greater omentum;
- Free taeniae - positioned on the anterior side of the intestine and are not attached to any structure.
All taeniae contain smooth muscle cells. Contractions of muscle fibers cause shortening of the large intestine wall, leading to the formation of the previously described segmented sacs (haustra) between the taeniae. The haustra give a segmented appearance to the large intestine, and they are more pronounced towards the sigmoid colon while often absent in the cecum.
At the sites where two haustra meet, crescent-shaped folds called the semilunar folds can be found. They are made of the mucosal and submucosal layers of the intestinal wall.
The epiploic appendices are found along the entire length of the large intestine. However, they are more pronounced in the distal parts of the colon, and there are particularly many of them on the surfaces of the transverse and sigmoid colon. The rectum, cecum and vermiform appendix usually lack epiploic appendices.
Large intestine parts
The large intestine is composed of several smaller parts. Overall, it can be subdivided into seven portions: cecum with the vermiform appendix, ascending colon, transverse colon, descending colon, sigmoid colon, rectum and anal canal. The ascending, transverse, descending, and sigmoid parts form the middle and also the largest section of the large intestine - the colon.
Cecum
The cecum is the first part of the large intestine located between the ileum and ascending colon in the right iliac fossa close to the anterior abdominal wall. It is around 2.4 inches (6 cm) long and resembles a blind pouch that is wider than it is long. The cecum starts at the distal end of the ileum as its continuation below the level of the ileocecal junction.
The cecum is considered an intraperitoneal organ, as the peritoneum covers it on all its sides. However, it has no mesentery and is rather mobile than fixed. The cecum usually contains all the characteristic features of the large intestine, except the epiploic appendices.
The cecum functions as a reservoir for the chyme coming from the small intestine, and it also participates in the absorption of the remaining water and electrolytes. Besides the mentioned functions, the cecum provides lubrication of the feces as it contains mucus-producing cells. Also, it participates in cellulose digestion as it contains bacteria that decompose plant-based food rich in cellulose.
At the ileocecal junction, the terminal ileum protrudes the posteromedial wall of the cecum, forming a mucosal eminence called the ileal papilla. The ileal papilla contains a small opening called the ileal or ileocecal orifice, through which the ileum connects with the cecum.
The ileal orifice is surrounded by two horizontal folds called lips. The upper is the superior ileocolic lip, while the lower is the inferior ileocecal lip. Both lips fuse around the orifice forming the ileocecal valve that works as a functional sphincter.
At the sides where both lips merge, they form narrow membranous ridges called the frenula (sing. frenulum). The ileocecal valve prevents the intestinal content backflow from the large intestine into the small intestine. It also controls the content flow from the ileum to the cecum.
Vermiform appendix
The vermiform appendix is a narrow tube-like structure with a blind end. The Latin word vermiform actually means "worm-like in form" because its shape resembles that of a worm. It is usually 2.5 - 4 inches (6 - 10 cm) long. However, the vermiform appendix is quite variable in its length, and it can range from 0.8 to 8 inches (2 - 20 cm). It contains massive amounts of lymphoreticular tissue, and therefore, it primarily provides immunological function.
The appendix extends from the posteromedial wall of the cecum, usually 0.4 - 1.2 inches (1 - 3 cm) below the ileocecal junction. Along with the cecum, it is also situated in the right iliac fossa, but its distal tip can extend as far as the liver and its location can be quite variable. The appendix is an intraperitoneal organ, and it has a triangular-shaped mesentery called the mesoappendix. It attaches the vermiform appendix to the terminal ileum and is derived from it.
Usually, the vermiform appendix has a retrocecal position, meaning it is located behind the cecum. Sometimes it can descend towards the lesser pelvis and pass even below the linea terminalis. In that case, its location is termed pelvic or caudal. It can rarely be subcecal (below the cecum) or preileal (in front of the terminal ileum).
Clinical note: The vermiform appendix can be palpated through the abdominal wall in the lower right quadrant of the abdomen in a site called McBurney’s point. If an imaginary line is drawn from the anterior superior iliac spine to the umbilicus, McBurney’s point is located one-third of the distance laterally. Tenderness or pain localized at this point or near it can signify appendicitis - inflammation of the appendix.
Colon
The colon is the longest and most prominent portion of the large intestine extending between the cecum and rectum. It has four main parts known as the ascending, transverse, descending and sigmoid colon. The ascending colon and descending colon both lie behind the peritoneum (retroperitoneally), but the transverse and sigmoid colon are intraperitoneal organs, meaning the peritoneum completely wraps them.
Ascending colon
The ascending colon is the first part of the colon that starts right above the ileocecal junction. It is a continuation of the cecum, extending on the right side of the abdominal cavity in the superior direction towards the liver. When reaching the right lobe of the liver, the ascending colon makes a sharp turn to the left, creating the right colic flexure (also called the hepatic flexure). The right colic flexure marks the junction between the ascending and transverse colon.
The ascending colon is related to various structures. Posterior to it lies the iliac fascia, quadratus lumborum muscle, iliolumbar ligament, transversus abdominis muscle, and renal fascia.
Several important neurovascular structures cross the anterior surface of the quadratus lumborum muscle; therefore, they are also located posterior to the ascending colon, including the lateral femoral cutaneous nerve, ilioinguinal nerve, iliohypogastric nerve, and the fourth lumbar artery. The anterior and lateral surfaces of the ascending colon are covered by the peritoneum.
Posterior to the right colic flexure lies the right kidney. The posterior aspect of the right colic flexure is not covered by the peritoneum. Therefore, it is in direct contact with the renal fascia. The right lobe of the liver is located superiorly, the fundus of the gallbladder lies anteromedially, and the descending part of the duodenum is situated medially to the flexure.
Transverse colon
The transverse colon is the longest and most mobile part of the entire large intestine. It crosses the upper aspect of the abdominal cavity from right to left. It begins at the right colic flexure as a continuation of the ascending colon and ends at the left colic flexure, transitioning into the descending colon.
The left colic flexure (also called the splenic flexure) is found on the left side of the upper abdomen at the level of the lower aspect of the spleen. It is usually more superior, less mobile and has a more pronounced angle than the right colic flexure. The phrenicocolic ligament attaches it to the diaphragm. The left kidney and tail of the pancreas lie behind the flexure.
Like the ascending colon, the transverse colon is also related to various structures. Superior to it are such anatomical structures as the liver, gallbladder, greater curvature of the stomach and gastrocolic ligament. Posteriorly, it is suspended from the parietal peritoneum of the posterior abdominal wall by a mesentery – the transverse mesocolon. The root of the mesentery passes along the inferior border of the pancreas and fuses with the parietal peritoneum.
Descending colon
The descending colon extends downward on the left side of the abdominal cavity from the left colic flexure towards the iliac crest, where it further continues as the sigmoid colon. The descending colon is a retroperitoneal organ, and it is typically immobile. However, around 33% of individuals can have a short mesocolon, and in that case, the descending colon can be slightly mobile.
Posterior to the descending colon is the renal fascia, as well as the quadratus lumborum, transversus abdominis, iliacus and psoas major muscles. Several neurovascular structures are also located posterior to the descending colon, including the subcostal arteries, veins and nerves, fourth lumbar artery, iliohypogastric, ilioinguinal, lateral femoral cutaneous, femoral and genitofemoral nerves. In contrast, the greater omentum and jejunum loops are situated anterior to the descending colon.
Sigmoid colon
The sigmoid colon is a continuation of the descending colon, and, at the same time, it is the fourth and final part of the colon. It starts at the level of the iliac fossa of the greater pelvis, then makes a curve and forms an S-shape loop. And finally, at the third sacral vertebra (S3) level, it transitions into the rectum, and this transition site is known as the rectosigmoid junction.
The rectosigmoid junction is also a site where the epiploic appendices and taenia coli terminate. It can be found approximately 6 inches or 15 cm from the anus.
The sigmoid colon is quite mobile because it has a long mesentery called the sigmoid mesocolon. The root of the mesentery has an inverted letter “V” shape, and it attaches the sigmoid colon to the posterior abdominal and pelvic walls.
Posterior to the sigmoid colon are the left internal iliac and gonadal vessels, left ureter, piriformis muscle, sacrum, and the sacral plexus. Lateral to the sigmoid colon are the left external iliac vessels, left ovary in females or ductus deferens in males, obturator nerve, and the lateral pelvic wall. Anterior and inferior to the sigmoid colon is the urinary bladder in males and the uterus and urinary bladder in females. The loops of the ileum lie on the right side of the sigmoid colon and superior to it.
Rectum
The rectum is the final and most distal part of the large intestine that connects the sigmoid colon with the anal canal. It is approximately 4.8 - 5.9 inches (12 - 15 cm) long and is rather fixed than mobile. The primary function of the rectum is the temporary storage of feces.
The rectum is a continuation of the sigmoid colon, beginning at the level of the third sacral vertebra (S3). This connection between the rectum and the sigmoid colon is called the rectosigmoid junction. The rectum ends at the perineum. As it passes through the puborectalis of the levator ani muscles (a muscle group forming the pelvic diaphragm), it continues as the anal canal.
The course of the rectum is marked by two major anteroposterior flexures - sacral and anorectal - and three additional lateral flexures that are formed by the submucosal transverse folds and are known as the valves of Houston.
Unlike the sigmoid colon, the rectum lacks haustra, taeniae coli, semilunar folds and epiploic appendices. The length of the proximal diameter of the rectum is similar to the sigmoid colon. It enlarges distally and forms a dilation called the rectal ampulla that further transitions to the anal canal at the level of the levator ani.
The rectum can be subdivided into three portions based on its relation to the peritoneum. The proximal third has an intraperitoneal location, and the peritoneum covers this portion anteriorly and laterally. The middle one-third is only covered anteriorly, and therefore, it lies retroperitoneally. And finally, the lower third of the rectum lies under the pelvic diaphragm. It is not covered by the peritoneum and has an extraperitoneal position.
The rectum is the most posterior positioned internal organ within the pelvic cavity, and the following structures are located posterior to it: sacrum and coccyx, anococcygeal ligament, presacral fascia, piriformis, levator ani and coccygeus muscles, median sacral, lateral sacral and superior rectal arteries, ganglion impar, lower sacral spinal and coccygeal spinal nerves, and the sacral parts of the sympathetic trunks. Laterally to the rectum lie the lateral rectal ligament, middle rectal artery, pararectal fossa, levator ani and coccygeus muscles and the inferior hypogastric plexus.
Anterior relations depend on gender. However, anterior to the rectum of both genders are the sigmoid colon and coils of the small intestine (ileum). In men, anterior to it is the rectovesical pouch, base of the urinary bladder, ampulla of the ductus deferens, seminal vesicles, terminal parts of the ureters, and the prostate. In women, anterior to the rectum are found the rectouterine pouch, uterus and posterior wall of the vagina.
Anal canal
The anal canal is the terminal part of the large intestine and the entire gastrointestinal tract. The anal canal is approximately 1 - 1.6 inches (2.5 - 4 cm) long. It is a continuation of the rectum, and it begins distally from the anorectal flexure when the rectum reaches the pelvic diaphragm and passes through the puborectalis of the levator ani muscle. The connection between the rectum and anal canal is called the anorectal junction.
The anal canal ends with an opening called the anus that connects the lower gastrointestinal tract with the external environment. From the anorectal junction, the anal canal descends in the posterior direction, and within the perineum, it is found in the anal triangle between the perineal body and the anococcygeal ligament. Like the distal one-third of the rectum, the anal canal also lies extraperitoneally. Its primary functions include the defecation and maintenance of fecal continence.
As the anal canal is responsible for fecal continence, it is surrounded by two sphincters - the internal and external anal sphincters - that prevent the unwanted passage of feces. The internal anal sphincter circularly surrounds the upper two-thirds of the anal canal, and it is a thickening of the circular muscle fibers of the muscularis externa layer. The internal anal sphincter is involuntary, meaning its contractions are activated by the sympathetic nervous system and inhibited by the parasympathetic nervous system.
The external anal sphincter is a voluntary sphincter containing skeletal muscle fibers controlled by the somatic nervous system. It is closely related to the puborectalis of the levator ani, and together with the internal anal sphincter, all mentioned muscles form the anorectal sling. This sphincter attaches anteriorly to the perineal body and posteriorly to the coccyx by means of the anococcygeal ligament. Superiorly it merges with the puborectalis muscle.
Overall, the anal canal can be subdivided into two segments - superior (upper) and inferior (lower). Both are separated by a demarcation line called the dentate or pectinate line. It is an irregular zig-zagging line that demarcates the superior two-thirds of the anal canal from its inferior one-third. Both segments between the dentate line have a different embryological origin, and therefore the neurovascular supply for each part is not the same.
The upper part of the anal canal has several longitudinal mucosal folds called the anal columns (columns of Morgagni). The most distal ends of the anal columns merge, forming a horizontal row of mucosal folds termed the anal valves. The location of the anal valves corresponds to the dentate line. Above the valves and between two anal columns, small recesses filled with mucus called the anal sinuses (sinuses of Morgagni) are present.
Anterior, the anal canal relates to the perineal body, which separates it from the root of the penis in men and the vagina in women. Lateral to the anal canal are the ischioanal (ischiorectal) fossae containing adipose tissue. And finally, posterior to it is the tip of the coccyx that is linked to the anal canal by the anococcygeal ligament.
Large intestine histology
The wall of the large intestine consists of the following layers:
- Mucosa
- Submucosa
- Muscularis externa
- Serosa/tunica adventitia
There are a few histologic differences between the large and small intestines. Compared to the small intestine, the mucosa of the large intestine lacks villi, Paneth cells and circular folds (plicae circulares), while the intestinal glands (crypts of Lieberkühn) are longer and produce more mucus as they contain much more goblet cells.
The submucosal and muscular layers of the large intestine are similar to those of the small intestine. However, the outer muscular layer of the large intestine forms taeniae that are not present in the small intestine. Also, the muscularis externa of the large intestine tends to be thicker than that of the small intestine.
Mucosa
The mucosa (mucosal layer) is the inner layer of the large intestine that faces its lumen. It is thinner in the colon but becomes thicker and contains more blood vessels towards the rectum. The mucosal layer of the large intestine consists of three sublayers:
- Epithelium
- Lamina propria
- Muscularis mucosae
The epithelium lining the mucosa of the large intestine is simple columnar, except at the anorectal junction, where it transitions from the simple columnar to the stratified squamous epithelium. Besides the columnar intestinal epithelial cells, the epithelium also contains goblet cells that secrete mucus, enteroendocrine cells producing hormones and rare microfold cells (M cells) that are specialized intestinal epithelial cells overlying the gut-associated lymphoid tissue (GALT) located below the epithelial layer. M cells ingest and transport antigen cells.
The columnar intestinal epithelial cells have an absorptive function. Their apical ends are covered by small projections called microvilli that are shorter than those of the small intestine. The mucus-producing goblet cells within the large intestine are more numerous compared to the small intestine. They gradually increase in numbers towards the rectum.
The intestinal mucosal glands (crypts of Lieberkühn) are simple tubular glands that are straight, unbranched and lined largely with goblet cells. They project deeper into the lamina propria, are located more closely and are more numerous in count than the intestinal glands of the small intestine. The intestinal glands are also lined by simple columnar epithelium. And besides the epithelial cells, they also contain other cells, including undifferentiated and neuroendocrine cells at their bases. However, they lack Paneth cells that are found within the intestinal glands of the small intestine. The crypts become shorter and shorter towards the anorectal junction and completely disappear at it.
The lamina propria is a layer of loose connective tissue providing structural support for the epithelium of the mucosa. It contains solitary lymphoid follicles that are less pronounced in the large intestine compared to the small intestine. The cecum, vermiform appendix and rectum have the most significant amounts of lymphoid follicles. Also, the lamina propria contains blood and lymph vessels, nerve fibers and immune cells.
The muscularis mucosae is the muscular layer of the mucosa located at the base of the mucosa. It separates the mucosa from the submucosa. The muscularis mucosae consists of smooth muscle cells. It is roughly eight to ten cells thick and is similar to the same layer of the small intestine. The muscularis mucosae of the large intestine becomes thinner and irregular towards the anorectal junction and disappears at it. Therefore, the lamina propria directly connects with the submucosa at the anorectal junction.
Submucosa
The submucosa or submucosal layer of the large intestine is formed by loose connective tissue infiltrated by such cells as the fibroblasts, macrophages, plasma cells, mast cells and lymphocytes. It contains many blood and lymphatic vessels, as well as nerve fibers and ganglion cells that form the submucosal nerve plexus (Meissner’s plexus). Overall, the submucosa of the large intestine is similar to the submucosal layer of the small intestine. However, the submucosa of the large intestine contains great amounts of submucosal veins forming plexuses at the anorectal junction.
Muscularis externa
The muscularis externa (also known as muscularis propria) lies beneath the submucosa and is arranged in two distinct layers containing smooth muscle cells - an outer longitudinal and an inner circular. Between both layers is the myenteric nerve plexus of Auerbach. The outer longitudinal layer is an irregular and incomplete layer organized into previously described muscular bands known as the taeniae coli.
The inner circular muscular layer, on the other hand, is thin and evenly spread throughout the large intestine. However, it gradually becomes thicker in the rectum and forms the internal anal sphincter at the upper aspect of the anal canal. Distally smooth muscle fibers are replaced by the skeletal muscle fibers that form the external anal sphincter.
Serosa/tunica adventitia
The serosa or serous membrane is the outermost layer of the intestinal wall formed by the visceral peritoneum. It consists of two sublayers: mesothelium, which refers to the simple squamous epithelium, and loose connective tissue beneath it. The serosa creates previously described epiploic appendices.
The peritoneum does not entirely cover the large intestine. The lower third of the rectum and dorsal aspects of the middle third of the rectum and the ascending and descending colon are covered by tunica adventitia instead of serosa. The tunica adventitia is the outermost loose connective tissue layer.
Neurovascular supply of large intestine
Arterial blood supply
The arterial blood supply of the large intestine mainly comes from the superior and inferior mesenteric arteries. The cecum, vermiform appendix, ascending colon, and proximal two-thirds of the transverse colon (all are derivatives of the midgut) are supplied by the following branches of the superior mesenteric artery:
- Ileocolic artery - provides arterial supply to the cecum, vermiform appendix and proximal ascending colon;
- Right colic artery - perfuses the ascending and transverse colon;
- Middle colic artery - supplies the transverse colon.
The distal third of the transverse colon, descending colon, sigmoid colon, rectum and proximal anal canal (the hindgut derivatives) are supplied by the branches of the inferior mesenteric artery:
- Left colic artery - perfuses the transverse and descending colon;
- Sigmoid arteries - provide blood supply to the sigmoid colon;
- Superior rectal artery - supplies the rectum and anal canal above the dentate line.
The internal iliac artery provides an additional arterial blood supply to the rectum and anal canal below the dentate line via its branch - the middle rectal artery. Also, the inferior rectal artery from the internal pudendal artery (a branch of the internal iliac artery) supplies both structures.
Note: During the embryological period, the gastrointestinal tract organs are derived from the primitive gut tube, which is divided into three portions: foregut, midgut and hindgut. Each of the portions is distinct in its embryological development and neurovascular supply. The foregut later develops into the esophagus, stomach, liver, gallbladder, pancreas, and the first part of the duodenum. The midgut develops into the rest of the duodenum, small intestine, and large intestine up to the proximal two-thirds of the transverse colon. And finally, the hindgut is the derivative of the remaining part of the large intestine up to the upper anal canal.
The superior and inferior mesenteric arteries communicate with each other via several anastomoses. One of them is formed between the middle colic artery and the left colic artery. However, it can also be created directly between the proximal superior mesenteric artery and the proximal inferior mesenteric artery. It is an inconstant anastomosis called the arc of Riolan or the central anastomotic mesenteric artery.
Also, all arteries of the large intestine form a unified anastomotic vessel called the marginal artery (also known as the marginal artery of Drummond). It runs parallel along the length of the large intestine from the ileocecal to the rectosigmoid junction. Since the main arteries forming the marginal artery are the branches of the superior mesenteric artery (ileocolic, right colic and middle colic arteries) and the inferior mesenteric artery (left colic artery), it is more pronounced along the cecum, ascending, transverse and descending colon. The sigmoid colon has a poorly developed marginal artery.
The marginal artery goes along the inner border of the large intestine, giving off numerous short branches that go towards the wall of the large intestine. These branches are called the straight arteries or vasa recta. The vasa recta can be further subdivided into the short vasa recta (short vessels) that run through the muscular layer and the long vasa recta (long vessels) that pass through the subserosa and muscular layer (muscularis externa), also supplying the epiploic appendices.
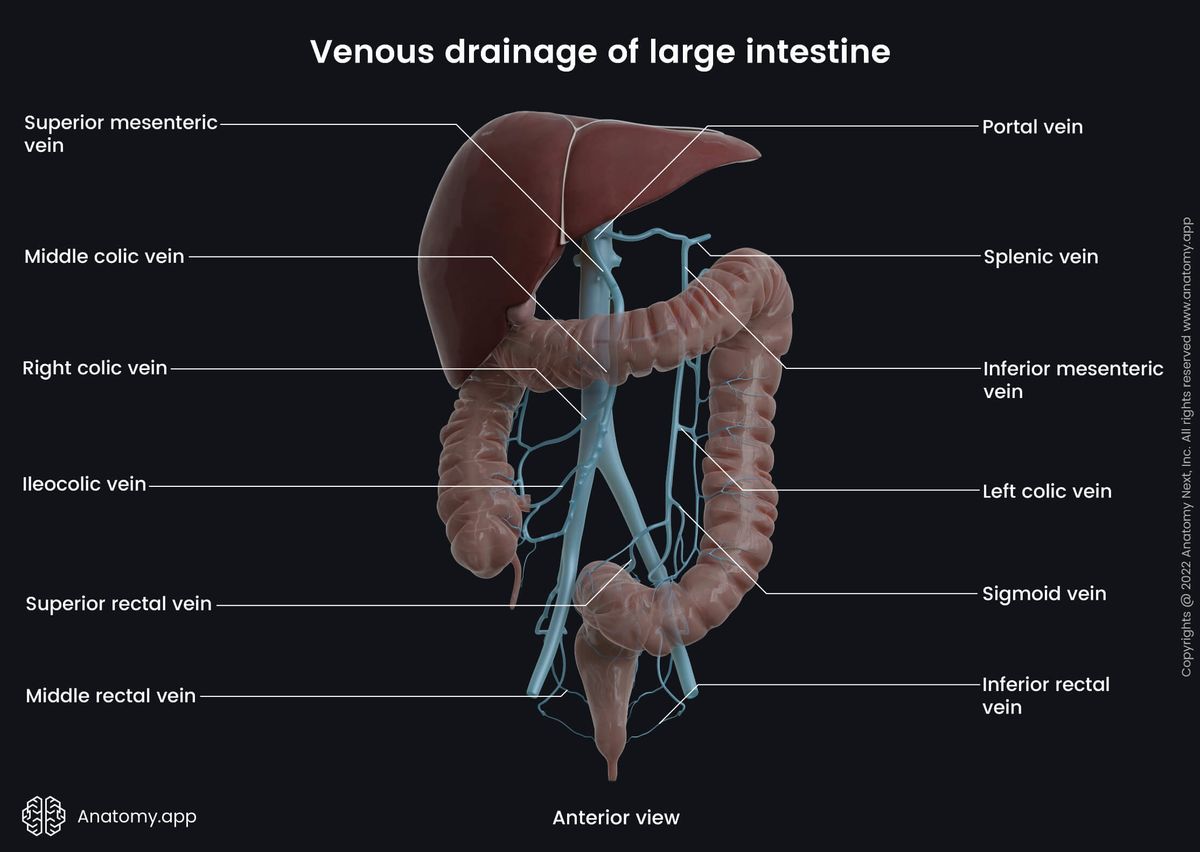
Venous drainage
The venous drainage of the large intestine is mainly provided by the hepatic portal system via the superior and inferior mesenteric veins. Additionally, venous blood collected from the rectum and anal canal drains into the systemic circulation via the internal iliac and internal pudendal veins.
Blood collected from the midgut derivatives (cecum, vermiform appendix, ascending colon and proximal two-thirds of the transverse colon) drains into the colic branches (ileocolic, right colic, middle colic veins) of the superior mesenteric vein.
In contrast, the hindgut derivatives (distal third of the transverse colon, descending colon, sigmoid colon, rectum and proximal part of the anal canal) are drained by the left colic, sigmoid and superior rectal veins into the inferior mesenteric vein. Further, the inferior mesenteric vein carries blood to the splenic vein, while the superior mesenteric vein joins the splenic vein and forms the hepatic portal vein.
As mentioned above, venous blood from the proximal rectum and anal canal above the dentate line is carried to the superior rectal veins that drain into the inferior mesenteric vein (part of the hepatic portal system). In contrast, the distal rectum and anal canal below the dentate line are drained via the inferior and middle rectal veins that carry blood to the internal pudendal and internal iliac veins (parts of the systemic circulation). Both systems (portal and systemic) are connected by numerous clinically important anastomoses.
Innervation
The innervation of the large intestine is very complex, and it comes from the intrinsic and extrinsic neurons forming intrinsic and extrinsic nervous systems, respectively. The intrinsic nervous system is located and formed within the intestine. It is interwoven in the wall of the large intestine and includes the enteric nervous system consisting of two nerve plexuses (Meissner’s and Auerbach’s plexuses) that provide local, autonomous functions. However, the intrinsic system also receives input from the extrinsic nervous system.
In contrast, the extrinsic nervous system includes efferent and afferent nerve fibers that primarily come from external sources. They originate from either the brain or spinal cord of the central nervous system. The extrinsic nervous system includes the autonomic nervous system with sympathetic and parasympathetic nerve fibers and the somatic nervous system providing only the sensory visceral afferent nerve fibers to the large intestine.
Enteric nervous system
The enteric nervous system, similar to the small intestine, comprises two nerve plexuses. Overall, they control intestinal motility (rhythmic movements of food through the intestines), smooth muscle cells, fluid exchange, mucosal secretion and local blood flow. The two plexuses are as follows:
- Submucosal plexus (also called the Meissner’s plexus) - located in the submucosa; innervates the muscularis mucosae layer and crypts of Lieberkühn, ensuring the secretion of the intestinal glands;
- Myenteric plexus (also known as Auerbach’s plexus) - situated in the muscularis externa between its circular and longitudinal muscle layers; innervates both layers and controls the motility of the intestinal wall.
Autonomic nervous system
The autonomic nervous system ensures sympathetic and parasympathetic innervation. Sympathetic innervation of the large intestine is provided by the thoracic, lumbar and sacral splanchnic nerves. The sympathetic fibers ensure vasoconstriction of the intestinal blood vessels and relaxation of the muscle cells in the intestinal wall.
The bodies of the preganglionic sympathetic neurons supplying the midgut derivatives (cecum, appendix, ascending colon and proximal two-thirds of the transverse colon) are located in the gray matter of the fifth to twelfth thoracic segments (T5 - T12) of the spinal cord. The axons of these neurons form the greater and lesser thoracic splanchnic nerves that travel to the celiac and superior mesenteric plexuses, where they synapse with the neurons of the celiac and superior mesenteric ganglia. The postganglionic axons reach the intestine and form the periarterial plexuses around the branches of the superior mesenteric artery.
The bodies of the preganglionic sympathetic neurons supplying the hindgut derivatives (distal one-third of the transverse colon, descending colon, sigmoid colon, rectum and proximal anal canal) are located in the gray matter of the first and second lumbar segments (L1 - L2) of the spinal cord. The axons of these neurons form the lumbar and sacral splanchnic nerves. The lumbar splanchnic nerves synapse with the neurons in the aortic and inferior mesenteric plexuses. The sacral splanchnic nerves synapse with the neurons in the superior and inferior hypogastric plexuses. The postganglionic axons form periarterial plexuses around the branches of the inferior mesenteric artery.
The parasympathetic innervation of the large intestine is ensured by the fibers of the vagus nerve (CN X). The parasympathetic fibers activate mucus secretion from the intestinal glands located within the mucosa and provide contractions of the smooth muscle cells situated within the intestinal wall. Branches of the vagus nerve innervate the midgut derivatives via the celiac and superior mesenteric plexuses. Branches of the vagus nerve that extend from the second to fourth sacral spinal cord segments (S2 - S4) innervate the hindgut derivatives via the pelvic splanchnic nerves that enter the inferior hypogastric plexus.
Somatic nervous system
The somatic nervous system contains visceral afferent fibers that send sensory information to the central nervous system. These fibers transmit information about distension and spasms of the intestinal wall. Transmission of sensations from the midgut is provided only by the fibers of the vagus nerve (CN X), while sensations from the hindgut are sent via the vagus nerve fibers that pass together with the lumbar and sacral splanchnic nerves. The anal canal below the dentate line is referred to as the cutaneous zone; therefore, it receives sensory nerve supply, and it comes from the pudendal nerve of the sacral plexus.
Lymphatic drainage
The lymphatic drainage of the large intestine is provided by lymphatic vessels and lymph nodes that mostly run along the course of the arteries. The lymph collected from the cecum, vermiform appendix, ascending colon, and proximal transverse colon are drained to the lymph nodes along the superior mesenteric artery. In contrast, the lymph from the distal transverse colon, descending colon, sigmoid colon and rectum drains into the lymph nodes around the inferior mesenteric artery.
There are four groups of lymph nodes related to the large intestine:
- Epicolic lymph nodes
- Paracolic lymph nodes
- Intermediate lymph nodes
- Preterminal (principal, preaortic) lymph nodes
The epicolic lymph nodes are small nodules located on the outer serosal surface of the large intestine, and sometimes they can even be found inside the epiploic appendices.
The paracolic lymph nodes are situated close to the artery of Drummond along the medial margin of the ascending and descending colon and at the mesenterial margins of the transverse and sigmoid colon.
The intermediate lymph nodes lie along the branches of the superior and inferior mesenteric arteries and have analogous names. They include the ileocolic, right colic, middle colic, left colic, sigmoid and superior rectal nodes.
The preterminal (principal, preaortic) lymph nodes are located along the course of the major arteries supplying the large intestine - superior and inferior mesenteric arteries.
The lymph collected from the cecum, vermiform appendix, ascending and transverse colon drains to the superior mesenteric nodes, while the descending colon, sigmoid colon and proximal part of the rectum drains to the inferior mesenteric nodes.
The lymph from the distal portion of the rectum is carried to the internal iliac and sacral lymph nodes. And finally, the anal canal above the dentate line is drained to the internal iliac nodes and inferior mesenteric nodes, while the lymph from the anal canal below the dentate line flows to the superficial inguinal nodes.
The lymph from the superior and inferior mesenteric lymph nodes drains into the intestinal lymph trunk before reaching the cisterna chyli. And finally, from the cisterna chyli, it is carried to the thoracic duct.
Large intestine functions
The main functions of the large intestine include the absorption of the remaining water and electrolytes from the gut contents, as well as the formation, propulsion and temporary storage of feces and subsequent participation in their expulsion in a process called defecation.
Also, the large intestine houses great amounts of gut microflora - bacteria and other microorganisms - that are responsible for such functions as vitamin K production and decomposition of indigestible components (cellulose) of chyme.
Intestinal motility (or movements) is ensured by rhythmic contractions of the smooth muscle cells found in the intestinal wall. These contractions are crucial for the formation of feces and their subsequent movements towards the rectum, from where they can be expelled in the external environment through the anal canal and anus.
References:
- Drake, R., Vogl, W., & Mitchell, A. (2019). Gray’s Anatomy for Students: With Student Consult Online Access (4th ed.). Elsevier.
- Gray, H., & Carter, H. (2021). Gray’s Anatomy (Leatherbound Classics) (Leatherbound Classic Collection) by F.R.S. Henry Gray (2011) Leather Bound (2010th Edition). Barnes & Noble.
- Moore, K.L., Dalley, A.F., Agur, A.M. (2018). Clinically Oriented Anatomy, 8th Edition, Lippincott Williams & Wilkins.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app